
Overview
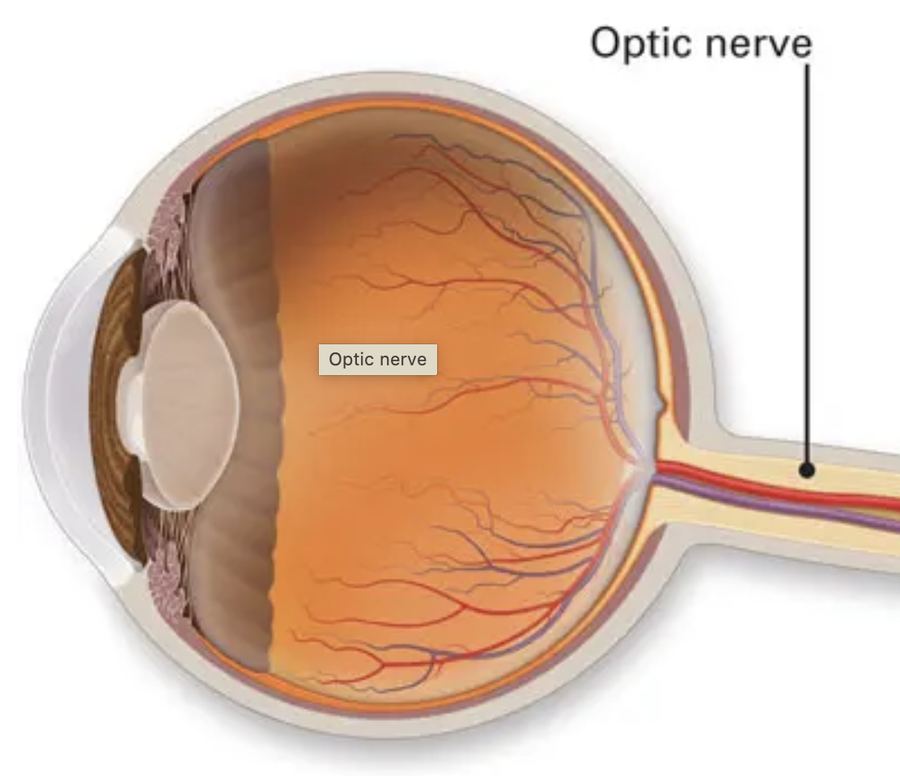
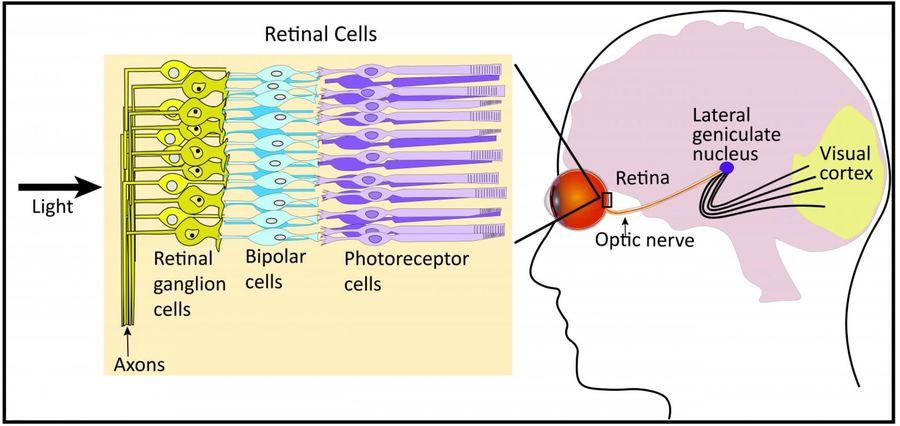
Glaucoma is a group of eye disorders characterized by progressive damage to the optic nerve (the nerve that carries visual signals from the eye to the brain).
Although elevated intraocular pressure (IOP) is the most familiar risk factor, glaucoma is increasingly understood as a neurodegenerative disease in which the retinal ganglion cells (RGCs) and their axons are damaged. This can occur in high-pressure states and even when IOP is in the "normal" range.
In practical terms: glaucoma results in irreversible damage to the cells of the inner retina — the RGC cells — which form connections to the brain via the optic nerve. This causes vision loss (especially peripheral/side vision first) and remains one of the leading causes of permanent blindness globally unless detected and treated early.
Why Call It a "Neurodegenerative Disease"?
Traditionally, glaucoma was thought of purely as an "eye pressure problem," but more modern research emphasizes that it fits many of the hallmarks of a neurodegenerative disorder. There is loss of specific neuronal populations — namely the retinal ganglion cells (RGCs) and their axons — similar to how Parkinson's disease involves the loss of neurons. The damage doesn't stop in the eye; changes have been documented in higher visual centers (for example the lateral geniculate nucleus) as the disease advances. In glaucoma, there is evidence of oxidative stress, glutamate excitotoxicity, mitochondrial dysfunction, axonal transport disruption, and altered neurotrophic support, all of which are features of neurodegeneration.
In other words, elevated IOP is a strong and modifiable risk factor, but the sensitivity of the neural tissue (its vulnerability to damage) is also critically important. Some eyes with "normal" IOP nonetheless develop glaucoma (so-called normal-tension glaucoma). Thus, thinking of glaucoma only as a mechanical pressure-driven disease is incomplete: it is better viewed as a multifactorial neurodegenerative optic neuropathy with eye pressure as one major modifiable factor.
Why Does This Happen?
Here's a simplified sequence of what happens in many cases of glaucoma (though many variations exist):
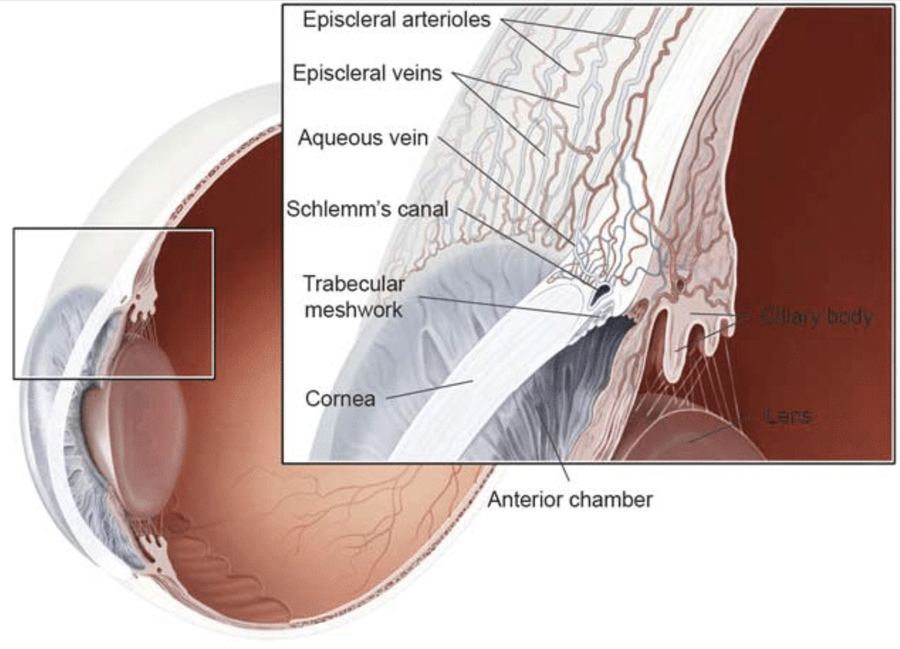
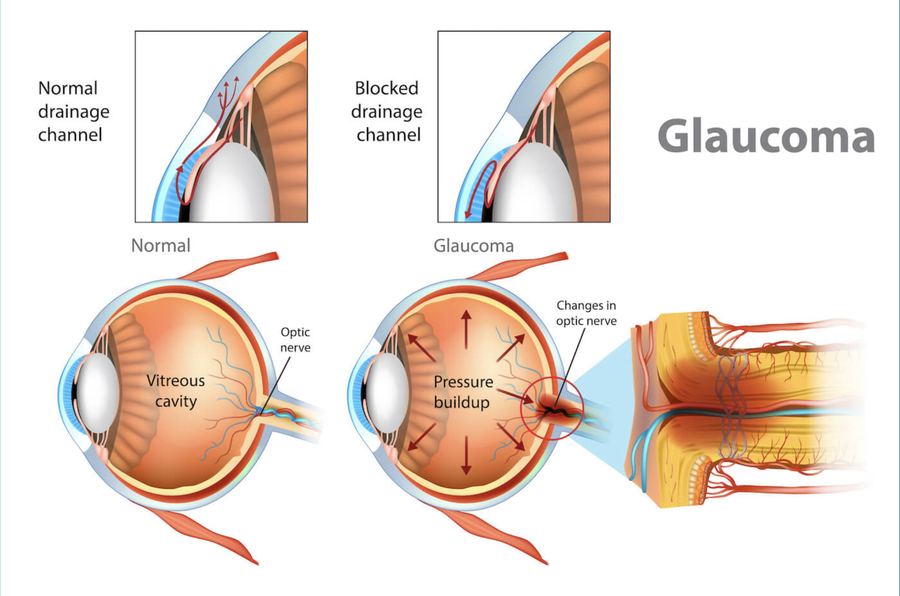
Fluid flow imbalance inside the eye: reduced outflow of the fluid inside the eye is a common cause of elevated eye pressure. This can be at the level of the intraocular filter called the trabecular meshwork (TM), which is the target of SLT laser therapy. After fluid passes through the TM it flows through Schlemm's canal and into the episcleral veins, which can also impede fluid escape from inside the eye.
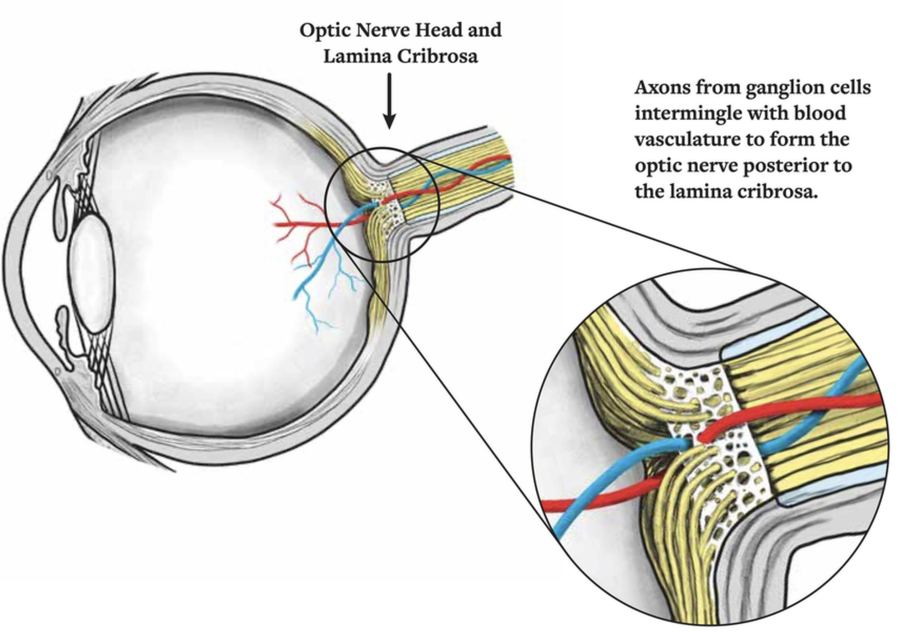
Elevated IOP and/or structural susceptibility: the optic nerve head (particularly the lamina cribrosa and the ganglion cell axons passing through it) is mechanically and/or biologically stressed. The lamina cribrosa may deform, impinging axons and micro-circulation. This is one of the newest major theories of how optic nerve damage occurs — an imbalance of pressures between the eye pressure and the brain's pressure, which meet at a point called the lamina cribrosa.
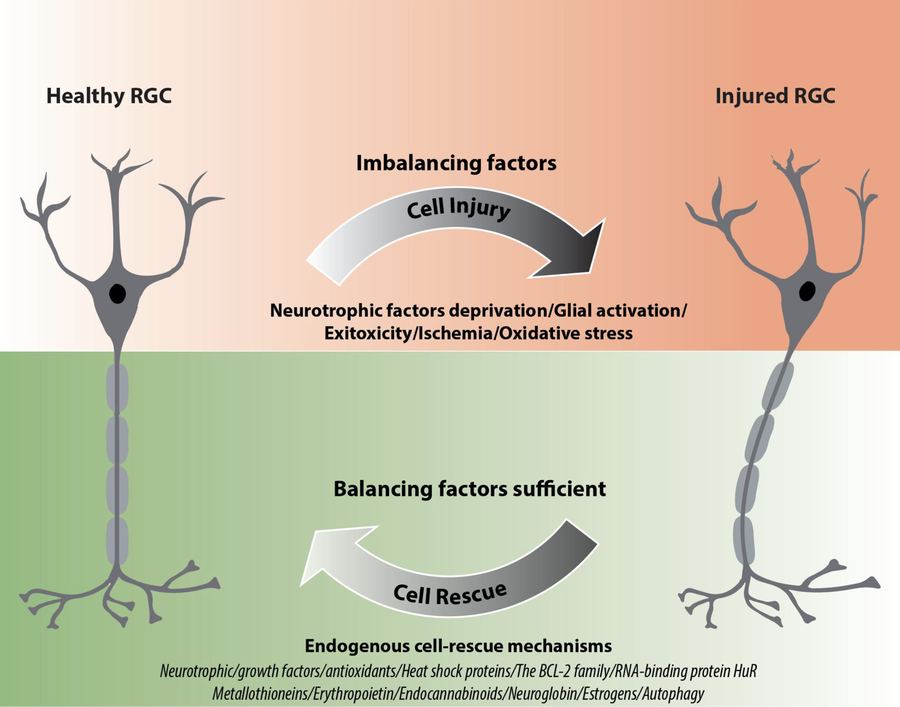
Axonal injury / impaired axonal transport: the RGCs lose axonal flow of nutrients and neurotrophins; mitochondria and cytoskeletons get damaged; oxidative stress, glutamate toxicity, and inflammatory responses may be triggered.
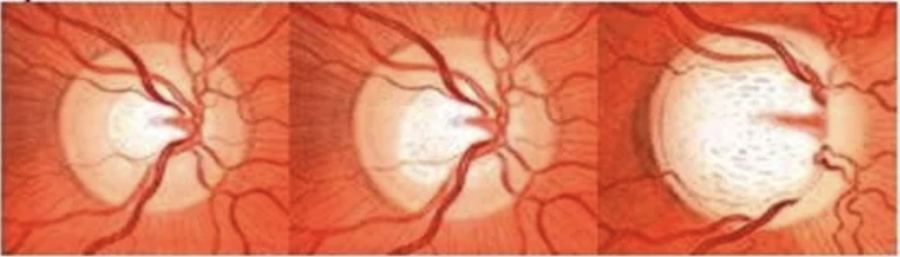
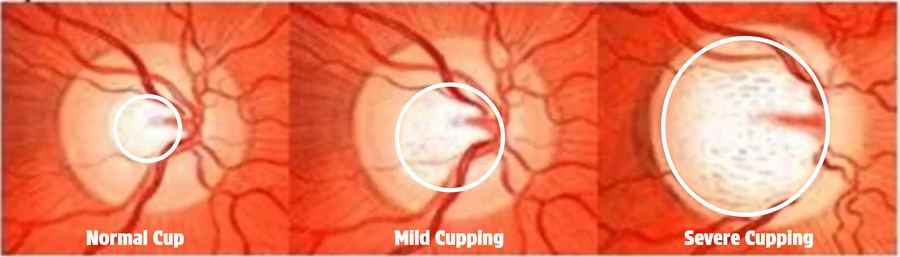
Retinal ganglion cell death and optic nerve degeneration: loss of RGCs leads to thinning of the nerve fiber layer, "cupping" of the optic disc, and ultimately loss of visual field.
Central nervous system changes: over time, neurodegenerative changes propagate into the brain's visual pathways, illustrating the systemic neurodegenerative nature of the disease.
Because of this chain, two major axes matter in glaucoma: pressure/outflow (elevated IOP or impaired drainage of aqueous humor) and neural vulnerability (how sensitive the optic nerve and RGCs are to damage, for instance due to genetics, blood flow, mitochondrial health, or oxidative stress). There is an interplay between these two factors — some people can withstand higher pressures without damage, and others with "normal" eye pressures are damaged. It also depends on how much pressure and for what length of time.
Classification: Open-Angle vs. Angle-Closure (Narrow-Angle)
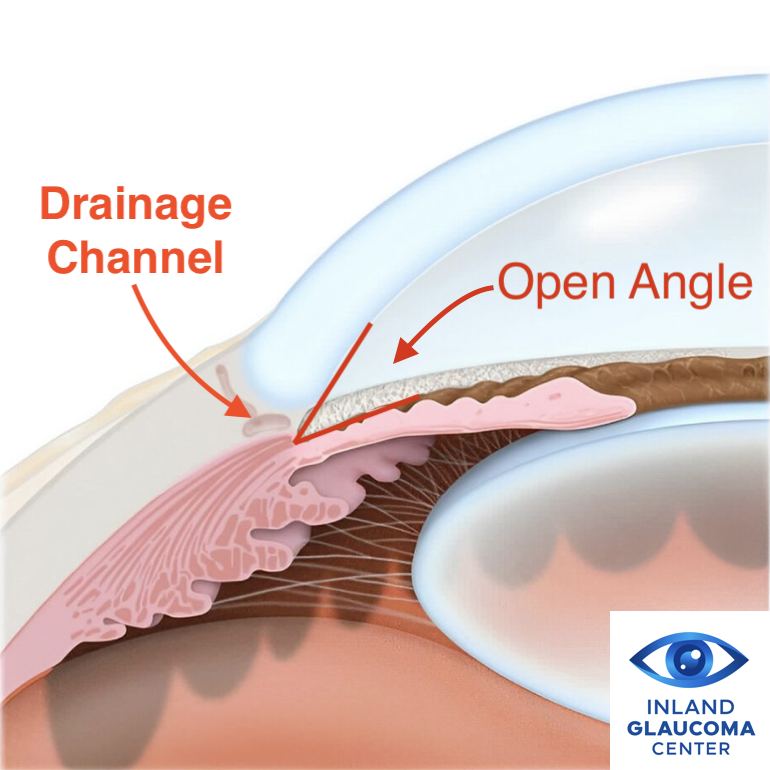
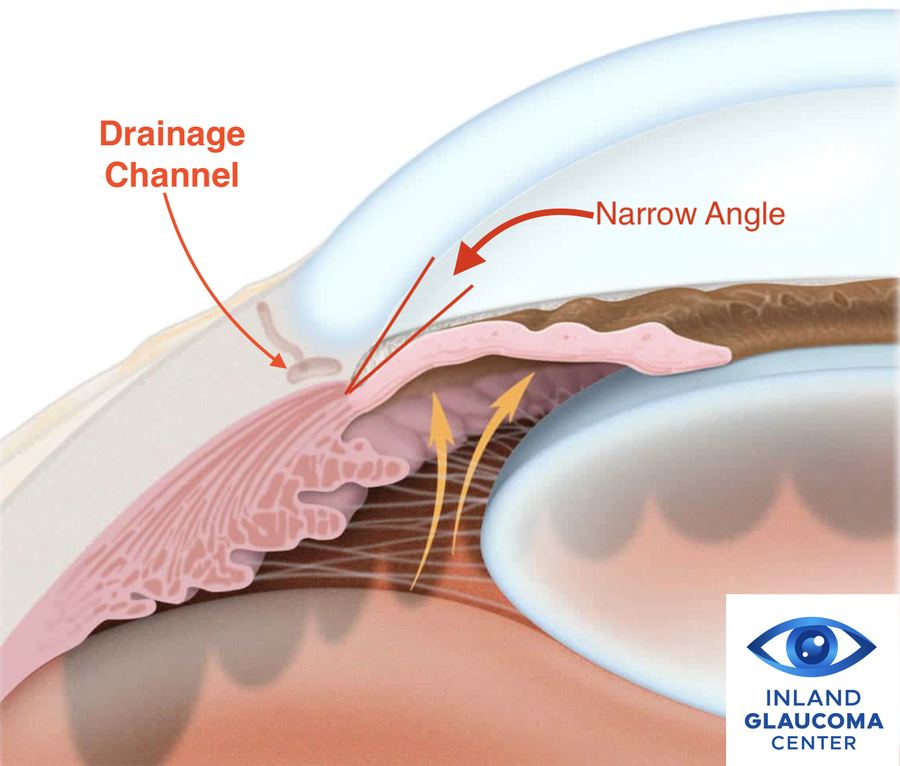
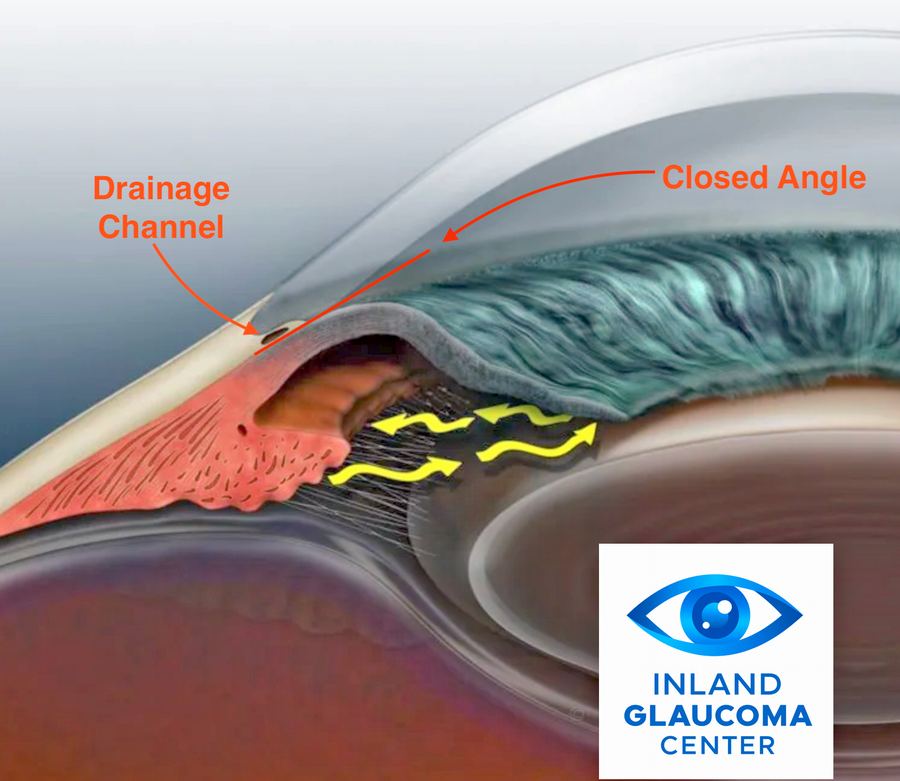
One of the basic ways clinicians classify glaucoma is by how the drainage angle of the eye (the anatomical space where aqueous humor leaves the eye via the trabecular meshwork) is involved.
Open-angle glaucoma: the angle between the iris and cornea is anatomically open (not mechanically closed or blocked), but drainage is still impaired (for instance trabecular meshwork dysfunction, debris, or pigment clogging). This is the most common type overall. The hallmark is slow, insidious onset of optic nerve damage, often without symptoms until significant vision loss has occurred.
Angle-closure (or narrow-angle) glaucoma: the drainage angle becomes narrowed or blocked (either suddenly or gradually), causing aqueous humor outflow to be drastically reduced, pressure to rise rapidly, and damage to the optic nerve to accelerate. This may present acutely (pain, red eye, halos around lights, nausea) or chronically (slow closure over time). Angle-closure glaucoma is less common than open-angle in many populations, but often needs more urgent intervention.
Primary vs. Secondary
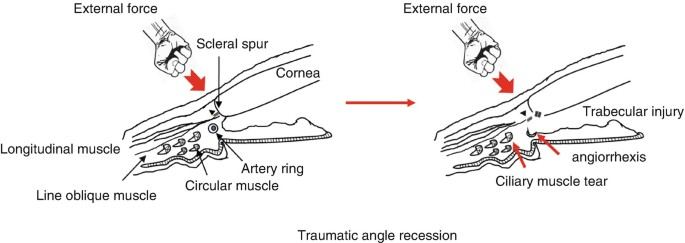
Primary glaucoma means there is no clearly identifiable cause for the drainage dysfunction (just the anatomical/developmental predisposition). Secondary glaucoma means there is an identifiable cause (trauma, inflammation, steroid use, exfoliation material, pigment dispersion, etc.) that contributes to the impaired outflow or increased pressure. Other causes of elevated pressure include the use of steroids either applied directly to the eye or systemically (by mouth or injection) — for example, someone using steroid eye drops or taking prednisone. A trauma to the eye, even many years ago, can damage the drainage structures of the eye, causing what's called angle recession glaucoma. Both primary and secondary types may present in open- or angle-closure forms.
Special Cases of Open-Angle Glaucoma
Pseudoexfoliation syndrome (pseudoexfoliation glaucoma): a systemic condition in which a protein-fibrillary material is deposited in the anterior segment of the eye (on the lens capsule, zonules, trabecular meshwork) and interferes with aqueous outflow, raising IOP and causing a secondary open-angle glaucoma. This type often progresses faster and produces higher IOP peaks than typical primary open-angle glaucoma. Genetic and environmental factors both contribute, and it's more common in individuals of Northern European descent.
Pigmentary glaucoma (pigment dispersion syndrome leading to glaucoma): pigment granules from the back of the iris break off and clog the trabecular meshwork, reducing outflow and raising IOP over time.
Steroid-induced glaucoma: use of corticosteroids (topical, intraocular, systemic) can increase IOP by altering the trabecular meshwork (increasing resistance to outflow) and lead to glaucomatous damage in predisposed individuals.
Uveitic glaucoma: inflammation of the anterior segment (uveitis) can damage outflow structures or cause secondary scarring or synechiae, raising IOP and causing optic nerve damage. Steroid treatment for uveitis can also precipitate glaucoma.
Angle-recession glaucoma: after ocular trauma, the drainage angle may be damaged (recession of the angle structures), leading to impaired outflow many years later.
Primary open-angle glaucoma (POAG): in many cases the source of outflow dysfunction is unknown (idiopathic), though there is a heritable component and anatomical/biological susceptibility.
Normal-tension glaucoma: although technically an open-angle type, this is where optic nerve damage occurs despite IOP never reaching "high" levels — emphasizing the "neural vulnerability" side of the equation.
These various sub-types show the spectrum of glaucoma: from "simple" elevated pressure from impaired drainage, to pressure-independent neural damage or combined mechanisms.
Genetic vs. Environmental (and Other) Etiologies
Genetic/heritable factors: many forms of glaucoma show familial clustering — a family history of glaucoma is a strong risk factor. Mutations in specific genes have been identified; for example, the gene MYOC (myocilin) is linked to some cases of juvenile-onset and adult-onset POAG. Genome/transcriptome studies show that glaucoma shares molecular pathways with other neurodegenerative disorders, involving cell adhesion, extracellular matrix remodeling, and calcium signaling. Some subtypes (e.g., pseudoexfoliation) have stronger genetic predispositions in certain populations. But penetrance (the chance that someone with the gene will get the disease) can be low and is influenced by other factors (environment, pressure, vascular supply, etc.).
Environmental/modifiable/other risk factors: elevated intraocular pressure (IOP) is one of the strongest modifiable risk factors — the higher the pressure (and the longer the duration), the greater the risk of optic nerve damage. Age: risk increases with advancing age. Race/ethnicity: some populations have higher risk (e.g., African descent, Asian descent for angle-closure). Anatomic factors: shallow anterior chamber, narrow drainage angle, lens thickness, etc. are predisposing for angle-closure. Vascular factors: impaired blood supply to the optic nerve, low ocular perfusion pressure, systemic hypotension, sleep apnea, etc. may contribute to neural vulnerability. Lifestyle factors: high myopia, eye trauma, steroid exposure, ocular surgery, inflammation (uveitis), exfoliation syndrome, pigment dispersion, etc. Systemic diseases: diabetes, hypertension, and other systemic vascular diseases may increase risk of optic nerve damage. Oxidative stress, mitochondrial dysfunction, and other metabolic/biological stressors may sensitize retinal ganglion cells to damage.
In short: genetic predisposition + anatomical/physiological modifiables + environmental/biological stressors = risk of glaucoma developing and progressing.

Putting It All Together: The Spectrum of Glaucoma
Glaucoma isn't one single disease but rather a spectrum of related disorders. At one end: relatively "simple" elevated pressure from poor drainage (classic open-angle or angle-closure), where controlling IOP may largely prevent damage. In the middle: mixed mechanisms — moderate elevation of pressure plus other insults (vascular, inflammatory, pigment deposition) leading to faster damage. At the other end: cases where IOP may be "normal" (normal-tension glaucoma) but the optic nerve is highly vulnerable and neurodegeneration proceeds because of non-pressure factors. Secondary glaucomas sit within this spectrum: pseudoexfoliation, pigmentary, steroid-induced, uveitic, trauma, etc. — each has a specific trigger in addition to the common final pathway of optic nerve damage.
Clinicians thus speak of glaucoma in terms of risk modification (lowering IOP, protecting the nerve) and neuroprotection (countering neural vulnerability). The neurodegenerative framing reminds us that simply lowering pressure may not fully arrest damage in all cases — one must also consider the health of the optic nerve and supporting structures.

Why Early Detection Matters
Because glaucomatous damage is irreversible: once retinal ganglion cells are lost and the optic nerve is damaged, we cannot regenerate those cells (at least not currently in standard practice). Vision loss tends to begin peripherally, so individuals often do not notice until advanced disease is present. By the time symptoms appear, significant damage may already have occurred. By detecting glaucoma early, intervening (via eye drops, laser, surgery, and addressing modifiable risk factors), and monitoring progression carefully, we can preserve useful vision for a lifetime.
Summary
Glaucoma is best thought of as a neurodegenerative optic neuropathy in which retinal ganglion cells and their axons die, often (but not always) driven by elevated intraocular pressure. There are two overarching anatomical categories: open-angle (most common) and angle-closure (or narrow-angle) glaucoma. Within those, a number of special sub-types exist (pseudoexfoliation, pigmentary, uveitic, steroid-induced, trauma/angle-recession, etc.) which reflect specific mechanisms of damage on top of the general one. Etiology is complex: genetic predisposition interacts with modifiable factors (IOP, anatomy, vascular health, inflammation, oxidative stress). Early detection and intervention are key because optic nerve damage is irreversible — the goal is to slow or stop progression rather than reverse it. Because glaucoma is a spectrum, treatment needs to be tailored: for some patients lowering IOP is enough; for others, we must address vascular/neural health, anatomical risk, and lifestyle/medical factors concurrently.
References
- Weinreb RN, Aung T, Medeiros FA. The pathophysiology and treatment of glaucoma: a review. JAMA. 2014;311(18):1901-1911. Casson RJ, Chidlow G, Wood JPM, Crowston JG, Goldberg I. Definition of glaucoma: clinical and experimental concepts. Clin Exp Ophthalmol. 2012;40(4):341-349. Calkins DJ. Critical pathogenic events underlying progression of neurodegeneration in glaucoma. Prog Retin Eye Res. 2012;31(6):702-719. Gupta N, Yucel YH. Glaucoma as a neurodegenerative disease. Curr Opin Ophthalmol. 2007;18(2):110-114. Nickells RW, Howell GR, Soto I, John SWM. Under pressure: cellular and molecular responses during glaucoma, a common neurodegeneration with axonopathy. Annu Rev Neurosci. 2012;35:153-179. Quigley HA, Broman AT. The number of people with glaucoma worldwide in 2010 and 2020. Br J Ophthalmol. 2006;90(3):262-267. Weinreb RN, Khaw PT. Primary open-angle glaucoma. Lancet. 2004;363(9422):1711-1720. Tham YC, et al. Global prevalence of glaucoma and projections of glaucoma burden through 2040: a systematic review and meta-analysis. Ophthalmology. 2014;121(11):2081-2090. National Eye Institute (NEI). Types of Glaucoma. U.S. National Institutes of Health. Updated 2023. BrightFocus Foundation. Understanding Secondary Glaucoma and Its Causes. 2023. American Academy of Ophthalmology (AAO) EyeWiki. Pseudoexfoliative Glaucoma. 2024. American Academy of Ophthalmology (AAO) EyeWiki. Pigmentary Glaucoma. 2024. Merck Manual Professional Edition. Overview of Glaucoma. 2023. Cleveland Clinic. Glaucoma: Symptoms, Causes & Treatment. 2024. Frontiers in Aging Neuroscience. Glaucoma as a neurodegenerative disease of the central visual system. Front Aging Neurosci. 2021;13:643685. Whitmore AV, Libby RT, John SWM. Glaucoma: thinking in new ways — a role for autonomous axonal self-destruction and other compartmentalised processes? Prog Retin Eye Res. 2005;24(6):639-662. Ritch R, Schlotzer-Schrehardt U. Exfoliation syndrome. Surv Ophthalmol. 2001;45(4):265-315. John SWM, Smith RS, Savinova OV, et al. Essential iris atrophy, pigment dispersion, and glaucoma in DBA/2J mice. Invest Ophthalmol Vis Sci. 1998;39(6):951-962. Fingert JH, et al. Myocilin gene mutations in primary open-angle glaucoma. Hum Mol Genet. 1999;8(5):899-905. Morrison JC, Johnson EC, Cepurna WO, Morrison JF. Understanding mechanisms of pressure-induced optic nerve damage. Prog Retin Eye Res. 2005;24(2):217-240. Leske MC. Open-angle glaucoma — an epidemiologic overview. Ophthalmic Epidemiol. 2007;14(4):166-172. Heijl A, Leske MC, Bengtsson B, et al. Reduction of intraocular pressure and glaucoma progression: results from the Early Manifest Glaucoma Trial. Arch Ophthalmol. 2002;120(10):1268-1279. Garway-Heath DF, Crabb DP, Bunce C, et al. Latanoprost for open-angle glaucoma (UKGTS): a randomised, multicentre, placebo-controlled trial. Lancet. 2015;385(9975):1295-1304. Yucel YH, Gupta N. Glaucoma of the brain: a disease model for trans-synaptic degeneration in the central nervous system. Br J Ophthalmol. 2008;92(9):1201-1204. Morgan JE. Circulation and axonal transport in the optic nerve. Eye. 2004;18(11):1089-1095. </content>