
What New Devices May Change the Way We Treat Glaucoma

For years, glaucoma surgery meant one of two things: traditional trabeculectomy, or tube shunt implantation. Both can be highly effective — but they are invasive and carry risks.
Over the last decade, a new category called MIGS (Minimally Invasive Glaucoma Surgery) has transformed care. These procedures are designed to lower eye pressure (IOP), reduce reliance on daily drops, and improve safety compared to older surgeries.
Now, in 2026, the surgical pipeline is expanding rapidly. Researchers and companies are developing new devices that target different fluid drainage pathways, aim to reduce scarring, and improve long-term predictability.
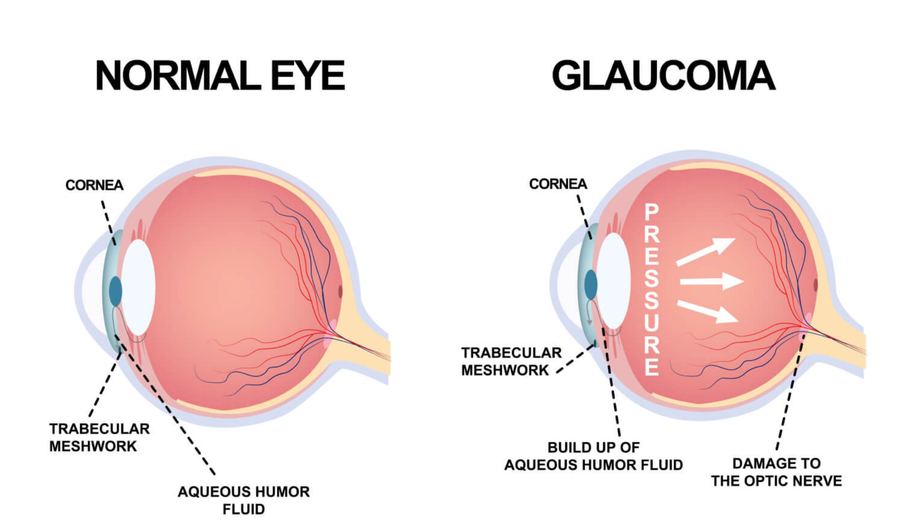
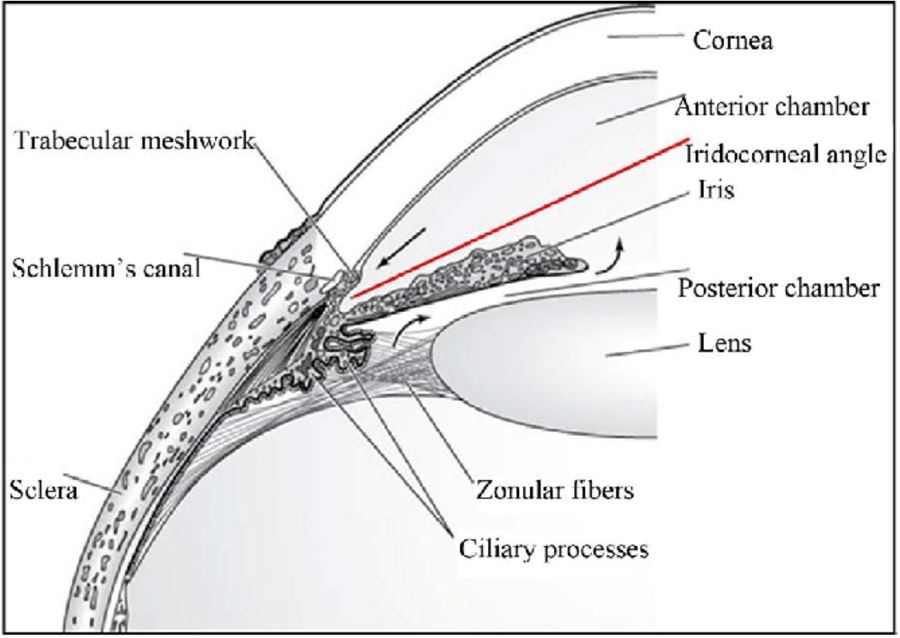
Glaucoma happens when fluid inside the eye doesn't drain properly, but we don't always know exactly where the blockage is. Some patients respond beautifully to a small trabecular stent while others barely see improvement, because resistance to outflow may exist in the trabecular meshwork, Schlemm's canal, the supraciliary space, or the subconjunctival space. The more tools surgeons have to target different pathways, the better we can personalize treatment.

Part 1: Next-Generation MIGS Devices
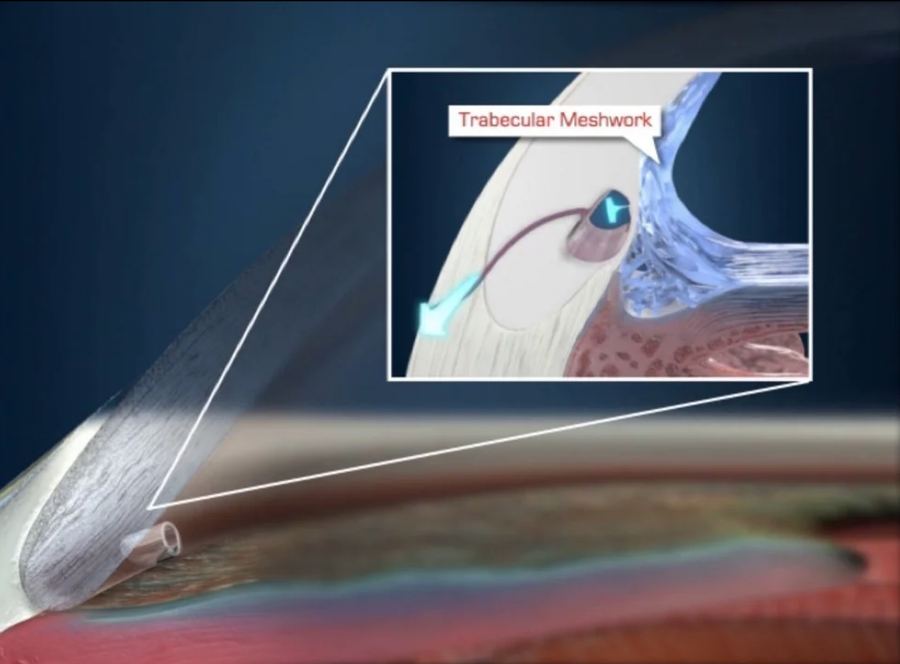
iStent Infinite (Glaukos): The iStent Infinite is a trabecular microbypass device that places three tiny stents into the eye's natural drainage system. It is currently approved for patients who have already failed other therapies, with trials underway to expand its use earlier in the disease process. The goal is to use small, targeted implants before patients require more aggressive surgery.
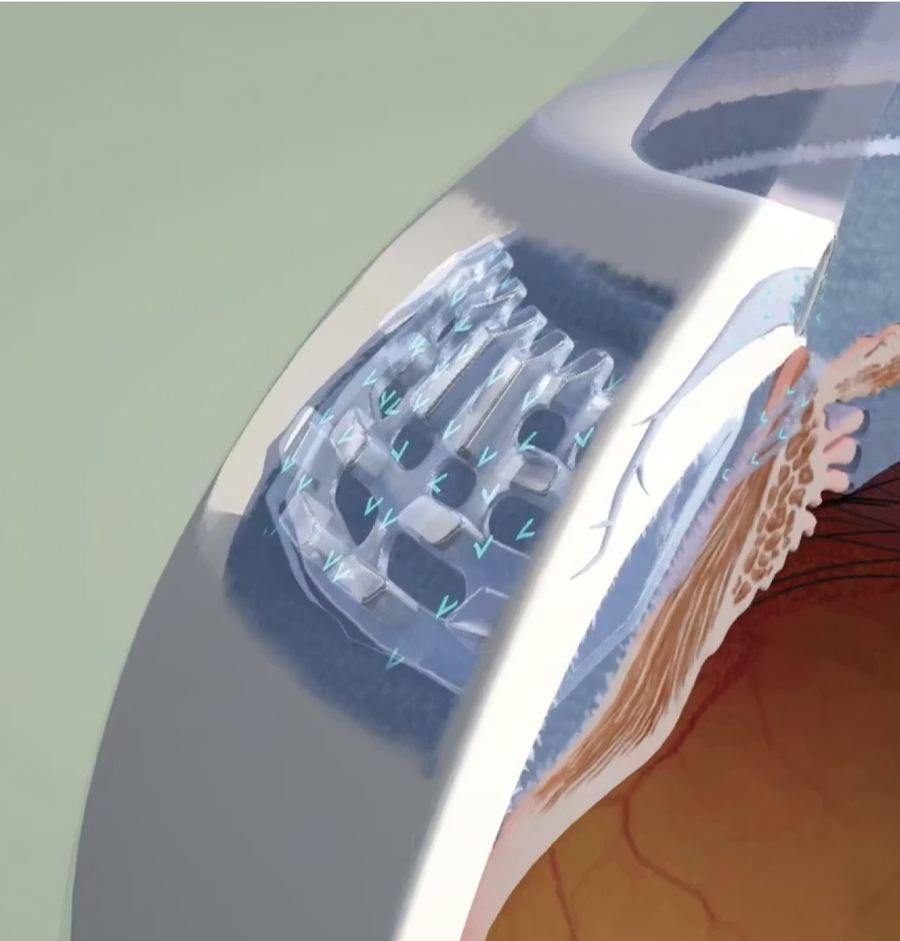
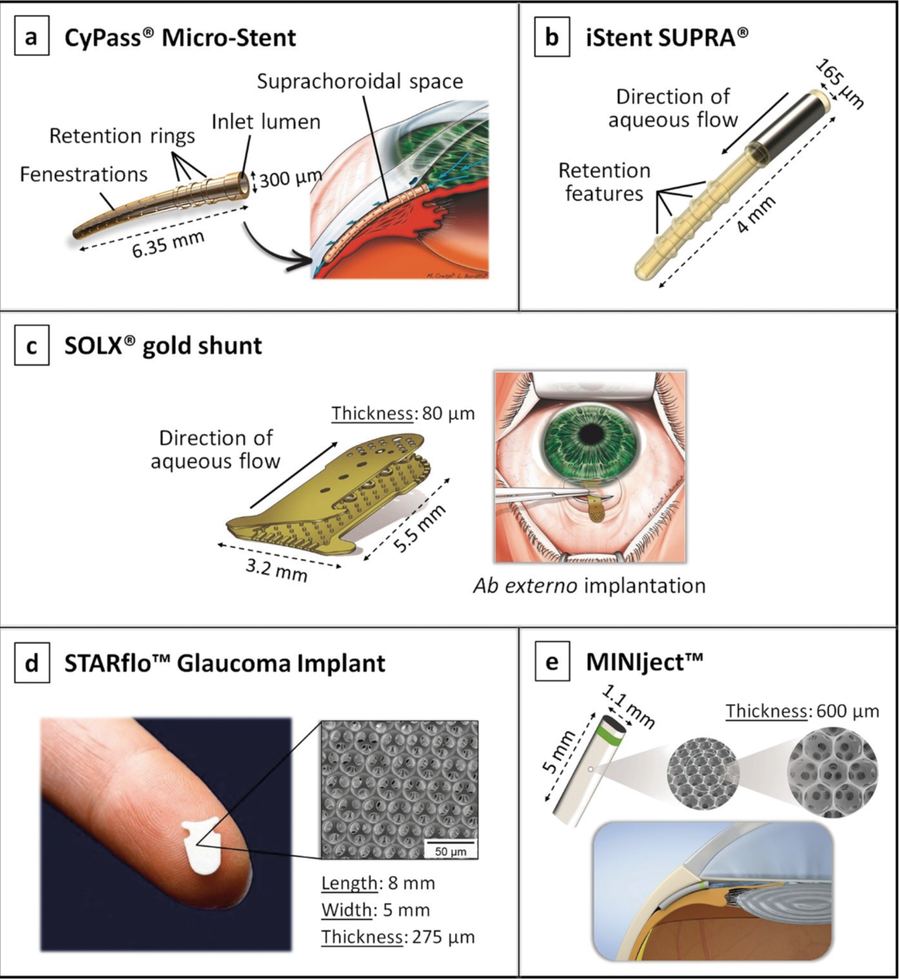
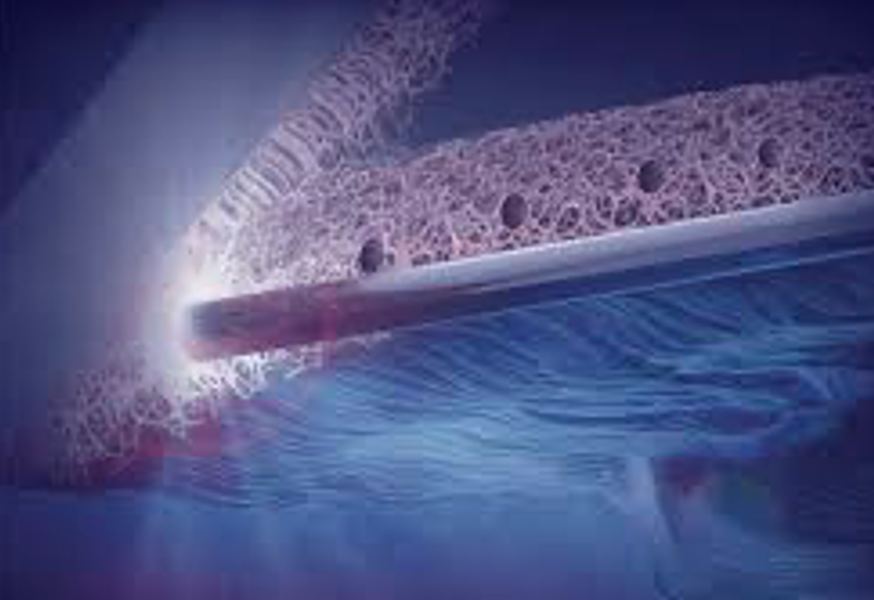
Supraciliary MIGS — MINIject (iStar Medical): The MINIject is designed to biointegrate into tissue and provide long-term pressure reduction. Five-year data outside the U.S. showed a 38% average IOP reduction, 80% of patients at or below 18 mmHg, and nearly one-third medication-free.
Supraciliary MIGS — Intercil (Ciliatech): The Intercil is a hydrophilic acrylic spacer placed between the ciliary body and sclera. Three-year data showed about a 33% IOP reduction, a 70% reduction in medication use, and no additional glaucoma surgeries required in studied patients. These devices are approved in Europe and moving toward U.S. trials.
Part 2: Microshunts & Blebless Innovations
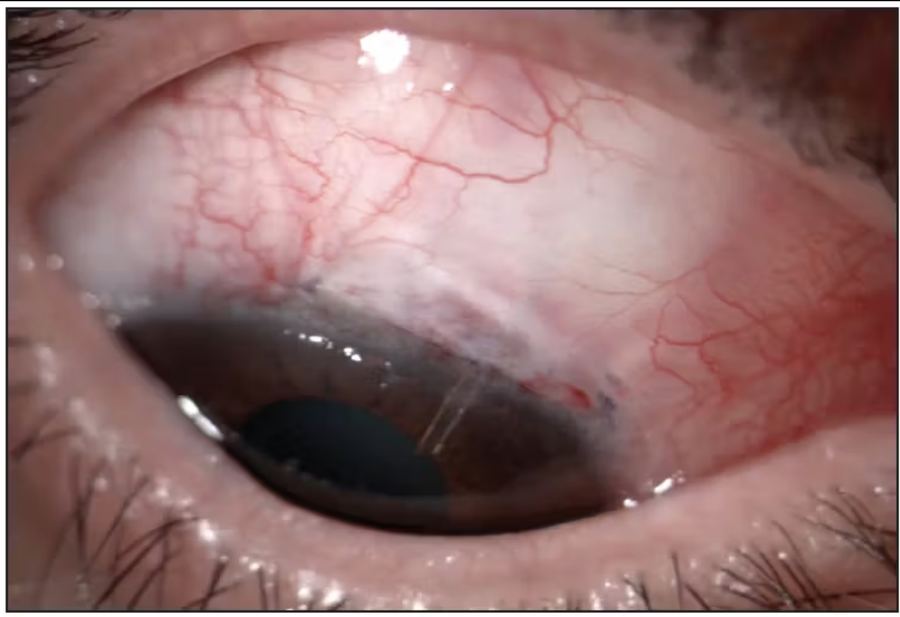
Preserflo Microshunt (Santen/Glaukos): Placed under the outer eye tissue (sub-Tenon's space) to form a low, diffuse bleb. One-year outcomes showed average IOP around 14 mmHg and 72% medication-free, with lower rates of certain complications compared to traditional trabeculectomy. However, in U.S. trials it did not outperform trabeculectomy in its primary endpoint, so it remains investigational in the U.S.
MIMS & MINT (Sanoculis): The MIMS (Minimally Invasive Micro Sclerostomy) creates a drainage channel without leaving an implant behind. One-year results showed a 38% pressure reduction and 60% of patients achieving very low pressures. The MINT variation creates multiple shallow drainage openings and showed strong success rates in early and moderate glaucoma. These represent a new category: implant-free filtration surgery.

Part 3: Laser-Based MIGS
Elios Laser Trabeculostomy: Creates tiny microchannels in the trabecular meshwork without leaving an implant. Eight-year follow-up data outside the U.S. showed sustained pressure reductions into the mid-teens. U.S. pivotal trials are underway.
ViaLuxe FLigHT Laser (Vialase): Uses OCT-guided femtosecond laser technology to create precise drainage channels. Early studies showed a 34% IOP reduction and 88% of treated eyes below 18 mmHg. It's already available in Europe and now entering U.S. trials.
Part 4: Next-Generation Drainage Implants
Traditional tube shunts are effective but can cause hypotony (pressure too low) and scarring. New implants aim to improve safety and reduce fibrosis.
Calibreye (Myra Vision): Titratable, meaning surgeons can adjust flow after surgery. Three-month data showed a 45% IOP reduction, 88% medication-free, and adjustable flow settings. This adjustability could reduce hypotony risk.
eyeWatch (Rheon Medical): Allows postoperative adjustment without another surgery. Three-year data showed sustained reductions and high overall success rates. It has received FDA Breakthrough Device designation.
VisiPlate (Avisi Technologies): Uses nonfibrotic material and multiple drainage channels to reduce clogging and scarring. Six-month pilot data showed about a 40% pressure reduction and strong medication reduction.

What This Means for Patients
The 2026 surgical pipeline shows several key themes: earlier intervention (doctors may intervene surgically earlier rather than relying on multiple drops for years); multiple outflow targets (surgeons can now target the trabecular meshwork, Schlemm's canal, the supraciliary space, and the subconjunctival space); improved safety (new devices aim to reduce hypotony risk, minimize scarring, and allow adjustable flow); and less "all-or-nothing" surgery (instead of one big surgery that must last forever, we now have stepwise options, adjustable implants, and combination approaches). This reduces both surgical stress and patient anxiety.

The Big Picture
Glaucoma surgery is no longer a last resort. With MIGS, laser microchannel procedures, supraciliary implants, and adjustable drainage devices, treatment is becoming more personalized, less invasive, more predictable, and focused on quality of life. Not every investigational device will reach approval, but the direction is clear: the surgical toolbox for glaucoma is expanding rapidly — and that's very good news for patients seeking better, safer, and earlier control of their disease.
If you have glaucoma and are struggling with drops or pressure control, ask your ophthalmologist what emerging options may soon be available. Book an appointment at Inland Glaucoma Center and let our board certified ophthalmologists in Upland help you. </content>